Limitations of Casemix and CMI Data as a Challenge to Evidence-Based and Equitable Health Financing Policy Advocacy
By dr. Yan Aslian Noor, M.P.H., FISQua
- Introduction
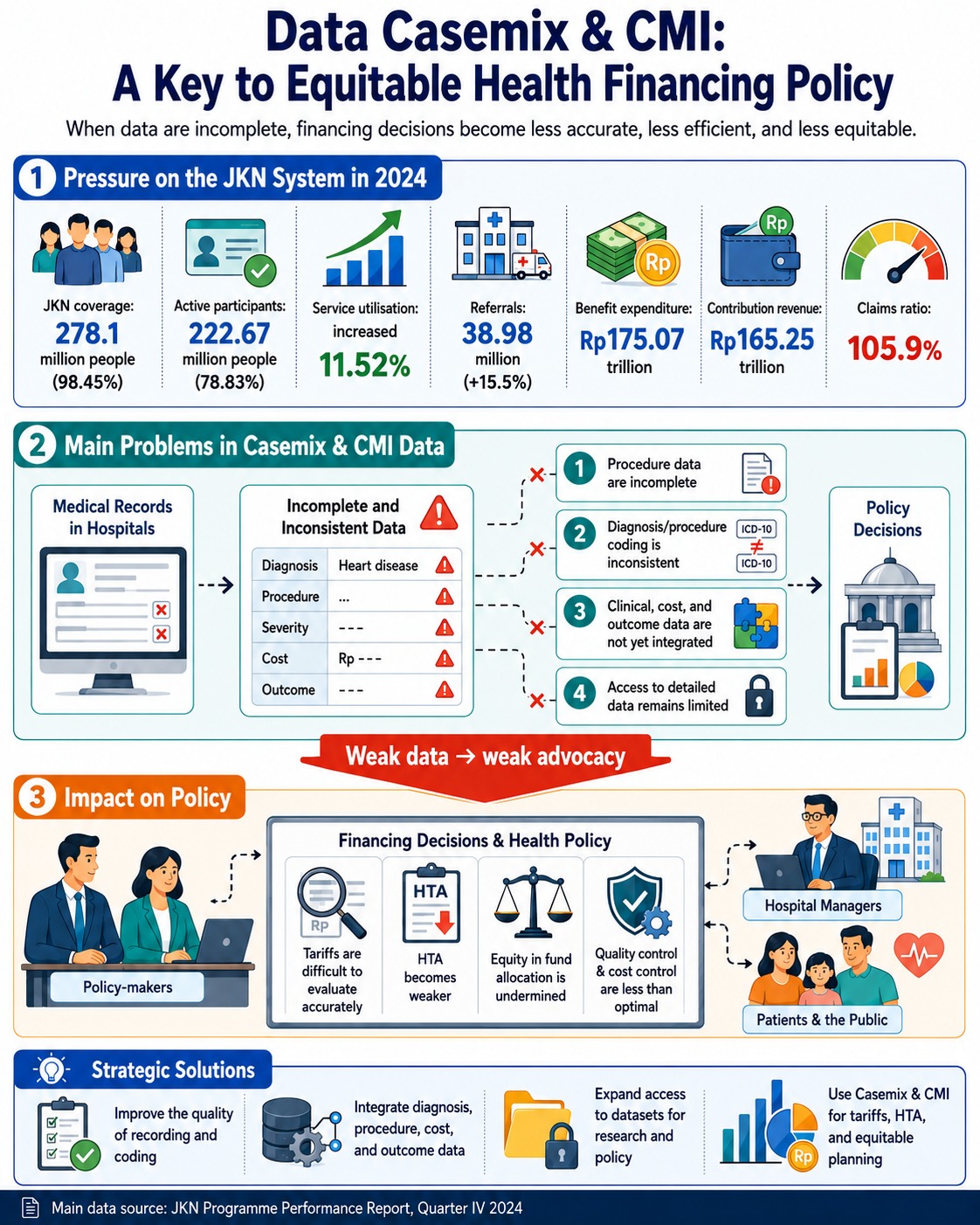
Indonesia’s National Health Insurance system, known as Jaminan Kesehatan Nasional (JKN), has become the country’s main instrument for achieving universal health coverage. According to the JKN Programme Performance Report, Quarter IV 2024, JKN membership as of 31 December 2024 reached 278.1 million people, or 98.45% of Indonesia’s population. This indicates that, administratively, JKN has almost covered the entire population. However, the same report also shows that active participants reached only 222.67 million people, or 78.83% of the population, while inactive participants totalled 55.43 million people, or 19.9% of all members. This highlights a gap between formal coverage and the actual functioning of health protection.
In the context of health financing, the challenge for JKN is not only to expand membership, but also to ensure that available funding is able to respond to increasingly complex healthcare needs. This is where casemix and the Case Mix Index (CMI) become highly relevant. Casemix describes the composition of patient cases based on diagnoses, procedures, severity levels, and resource requirements. CMI, meanwhile, reflects the average level of case complexity handled by a healthcare facility. The higher the CMI, the more severe and complex the cases being treated, and therefore the greater the need for funding, health professionals, medical equipment, and supporting services.
The problem is that casemix and CMI data are not always available in a complete, detailed, and accessible format for policy advocacy. In practice, one common issue is the absence of detailed procedure data, for example data based on ICD-9-CM, within analytical datasets. Yet procedure data are essential for assessing whether a service requires substantial funding, whether INA-CBG tariffs are adequate, and whether financing policies are fair for both patients and hospitals.
- JKN Utilisation Data: The Service Burden Is Increasing
JKN data for Quarter IV 2024 show a significant increase in healthcare service utilisation. As of 31 December 2024, service utilisation had increased by 11.52% compared with December 2023. The highest utilisation was recorded in Primary Outpatient Care (RJTP), with 512.52 million visits, an increase of 11% from the previous year. This was followed by Advanced Outpatient Care (RJTL) with 143.47 million visits, an increase of 13%; Advanced Inpatient Care (RITL) with 18.42 million admissions, an increase of 13%; and Primary Inpatient Care (RITP) with 2.95 million admissions, an increase of 23%. The number of referrals also rose from 33.75 million in 2023 to 38.98 million in 2024, an increase of 15.5%.
These figures show that the JKN service burden is not only large, but also continuing to grow. The increase in referrals to advanced care suggests that primary care still faces challenges in performing its role as a gatekeeper. From a casemix perspective, rising referrals and advanced care visits should be examined more deeply: are they driven by more complex cases, weaknesses in primary care, changing disease patterns, inefficient referral practices, or a genuine increase in the need for specialist services?
Without detailed casemix and CMI data, policy advocacy can only state that utilisation is increasing. It cannot yet answer more precise questions: which types of cases are increasing, how severe they are, which procedures absorb the most funding, and whether the financing provided is proportionate to the complexity of care.
- Benefit Expenditure Data: Financing Pressure Is Rising
From a financing perspective, the JKN Programme Performance Report, Quarter IV 2024 shows that benefit expenditure increased by 10%, from Rp158.9 trillion in 2023 to Rp175.07 trillion in 2024. The largest expenditure was for Advanced Inpatient Care (RITL) at Rp99.1 trillion, followed by Advanced Outpatient Care (RJTL) at Rp53.5 trillion, Primary Outpatient Care (RJTP) at Rp19.6 trillion, Primary Inpatient Care (RITP) at Rp1.96 trillion, and promotive-preventive services at only Rp0.9 trillion.
This composition is important for strengthening the analysis. First, JKN financing is heavily dominated by curative services, particularly hospital-based and advanced-level care. Second, allocation for promotive and preventive services remains very small compared with curative expenditure. Third, without complete casemix data, it is difficult to determine whether the increase in expenditure is caused by a higher number of cases, greater case complexity, tariff increases, changing disease patterns, or possible inefficiencies in service delivery.
The report also notes that RJTL benefit payments reached Rp53.5 trillion, an increase of 14% compared with the previous year. Within RJTL, the most frequent CBG group was “other minor chronic diseases”, with 78.47 million cases, followed by physical therapy and minor musculoskeletal procedures with 13.73 million cases, and dialysis procedures with 7.55 million cases. Meanwhile, RITL benefit payments reached Rp99.1 trillion, an increase of 8% from the previous year. The most common RITL cases included mild non-bacterial infections, mild caesarean section procedures, abdominal pain and gastroenteritis, and mild bacterial and parasitic infections.
These data show that the JKN system manages a very large volume of claims. However, aggregate CBG data alone are not sufficient to answer deeper policy questions. For example, in the case of dialysis, additional data are needed on primary diagnosis, comorbidities, treatment frequency, outcomes, cost per patient, and survival rates. For caesarean section cases, data are needed on clinical indications, severity, complications, length of stay, and regional variation. Without such details, health financing advocacy will struggle to distinguish between legitimate funding needs, potential inefficiencies, and clinical practice variations that require better control.
- JKN Financial Health and the Urgency of Casemix Data
Financing pressure is also reflected in the financial condition of the Health Social Security Fund. In 2024, JKN contribution revenue reached Rp165.25 trillion, or 103% of the Rp160.42 trillion target. However, actual benefit expenditure reached Rp175.07 trillion, leading to a decline in net assets of Rp7.31 trillion. The claims ratio reached 105.9%, meaning that benefit expenditure exceeded contribution revenue. The report explains that the claims ratio above 100% was caused by tariff growth and increased healthcare service utilisation, particularly in RJTL and RITL, which had not been matched by growth in contribution revenue.
This reinforces the urgency of using casemix and CMI data in policy advocacy. When the claims ratio has reached 105.9%, policy debate should not focus only on whether contributions need to be increased. It is also necessary to understand which components are driving expenditure growth, whether insured cases are becoming more complex, whether there are changes in severity, whether tariffs are appropriate, and whether some services may be less cost-effective.
The JKN report also states that the net assets of the Health Social Security Fund are projected to finance the programme for 3.38 months ahead, but the fund still faces a risk of deficit if the upward trend in benefit expenditure is not accompanied by improved contribution collection and other sources of income. In this situation, health financing advocacy requires data that are not only large in aggregate terms, but also analytically sharp. Casemix and CMI data can help determine whether financing should be directed towards tariff adjustment, strengthening primary care, improving referral control, revising benefits, or prioritising health technologies.
- Why Limitations in Casemix Data Hinder Advocacy
Limitations in casemix and CMI data hinder advocacy in several ways.
First, they weaken advocacy for tariff adequacy. Hospitals that manage complex cases require greater resources. However, without reliable CMI and severity data, it is difficult to prove whether INA-CBG tariffs for certain cases are too low, adequate, or too high. As a result, tariff debates can easily become subjective.
Second, these limitations hinder advocacy for fairness between hospitals and regions. National referral hospitals, hospitals in remote areas, and lower-class hospitals face different case burdens. If casemix data do not reflect the actual complexity of care, financing policies risk treating all facilities as if they carry the same burden. This may create inequities in funding.
Third, incomplete casemix data weaken Health Technology Assessment (HTA). HTA requires detailed information on diagnoses, procedures, costs, outcomes, and clinical benefits. If datasets do not include procedure details based on ICD-9-CM, it becomes difficult to assess the effectiveness and efficiency of a health procedure or technology. In a context where the JKN claims ratio has reached 105.9%, decisions on health technology financing must become increasingly selective and evidence-based.
Fourth, data limitations undermine quality control and cost control. The JKN Quarter IV 2024 report explicitly recommends strengthening governance, quality control, and cost control, especially because of the significant increases in visits and benefit expenditure in RJTL and RITL. However, quality and cost control cannot be carried out effectively if available data cannot show the relationship between diagnosis, procedure, severity, cost, and outcome.
- Data as a Foundation for Equitable Health Financing Advocacy
From an equity perspective, fair health financing does not mean that every facility receives the same amount of funding. Rather, funds should be allocated according to need and service complexity. Patients with chronic diseases, comorbidities, disabilities, catastrophic illnesses, or long-term care needs require different levels of financial support compared with patients with mild conditions.
JKN data show that chronic and advanced services absorb a substantial share of utilisation and expenditure. For example, RJTL recorded 78.47 million cases of other minor chronic diseases and 7.55 million dialysis procedures. These data can support advocacy for stronger health financing policies in chronic disease management, complication prevention, primary care strengthening, and continuity of care.
However, for advocacy to be sharper, aggregate data must be complemented by more detailed casemix data. For dialysis patients, for example, data are needed on age distribution, accompanying diagnoses, duration of treatment, complications, outcomes, and cost per episode. For chronic diseases, analysis is needed to determine whether financing is being absorbed by complications that could have been prevented through stronger primary care. In this way, advocacy does not merely demand additional funding; it also promotes better financing design.
- Conclusion: Strengthening Policy Through Better Data
JKN data for Quarter IV 2024 show that the system faces three major pressures: coverage is almost universal but active participation remains suboptimal; service utilisation is increasing sharply; and benefit expenditure has exceeded contribution revenue. Membership reached 278.1 million people, but active participants numbered only 222.67 million. Service utilisation increased by 11.52%, referrals rose by 15.5%, benefit expenditure reached Rp175.07 trillion, and the claims ratio reached 105.9%.
In this context, limitations in casemix and CMI data represent a serious barrier to evidence-based and equitable health financing policy advocacy. Without complete data on diagnoses, procedures, severity, costs, and outcomes, policy-makers will struggle to determine whether rising benefit expenditure is driven by legitimate medical needs, increasing case complexity, weaknesses in primary care, inefficiencies, or inappropriate tariffs.
Therefore, the advocacy agenda should not only focus on increasing the health budget. It should also prioritise strengthening the governance of casemix and CMI data. These data should be used as a foundation for tariff revision, HTA strengthening, health facility planning, referral control, quality evaluation, and the development of fairer health financing policies.
The table below presents key JKN indicators for 2024 that support the argument that limitations in casemix and CMI data may hinder evidence-based and equitable health financing policy advocacy.
Table 1. Summary of JKN Membership, Utilisation, and Financing Indicators in 2024 as a Basis for Health Financing Policy Advocacy
| Aspect | 2024 Data | Relevance to the analysis |
| JKN membership coverage | 278.1 million people / 98.45% of the population | Shows that JKN is almost universal administratively |
| Active participants | 222.67 million people / 78.83% of the population | Indicates a gap between coverage and active protection |
| Inactive participants | 55.43 million people / 19.9% of members | Strengthens the issue of membership sustainability |
| Total service utilisation | Increased by 11.52% | Shows utilisation pressure |
| Primary Outpatient Care (RJTP) | 512.52 million visits | Indicates a very large primary care burden |
| Advanced Outpatient Care (RJTL) | 143.47 million visits | Shows high demand for advanced care |
| Advanced Inpatient Care (RITL) | 18.42 million admissions | Directly linked to high expenditure |
| Referrals | 38.98 million, up 15.5% | Highlights gatekeeping and primary care effectiveness issues |
| Benefit expenditure | Rp175.07 trillion | Shows financing pressure |
| Contribution revenue | Rp165.25 trillion | Lower than benefit expenditure |
| Claims ratio | 105.9% | Indicates a risk to financial sustainability |
| Decline in net assets | Rp7.31 trillion | Indicates financial pressure on the Health Social Security Fund |
| Fund resilience | 3.38 months | Still financially sound, but at risk if expenditure continues to rise |
| RITL benefit payments | Rp99.1 trillion | The largest burden is in advanced inpatient care |
| RJTL benefit payments | Rp53.5 trillion | A major burden lies in specialist and advanced outpatient services |
| RJTL dialysis cases | 7.55 million cases | Relevant for HTA and chronic disease financing |
| Promotive-preventive services | Rp0.9 trillion | Very small compared with curative expenditure |
Source: Adapted from the JKN Programme Performance Report, Quarter IV 2024, covering membership, healthcare facility cooperation, service utilisation, benefit expenditure, contribution revenue, claims ratio, and the financial health of the Health Social Security Fund as of 31 December 2024.
The table shows that JKN has achieved very broad membership coverage, while at the same time facing rising service utilisation, increasing benefit expenditure, and growing pressure on financial sustainability. This further reinforces the importance of more detailed casemix and CMI data to assess case complexity, tariff adequacy, referral effectiveness, HTA priorities, and equity in health financing allocation.
References
BPJS Kesehatan. (2024). Launch of the BPJS Kesehatan Sample Data 2024: Data 2015–2023.
Centers for Medicare & Medicaid Services. (n.d.). Case Mix Index.
Dewan Jaminan Sosial Nasional/BPJS Kesehatan. (2024). JKN Programme Performance Report, Quarter IV 2024. Jakarta: DJSN and BPJS Kesehatan.
Ministry of Health of the Republic of Indonesia. (2024). Cross-Sector Coordination on National Health Accounts 2023.
Mendez, C. M., Harrington, D. W., Christenson, P., & Spellberg, B. (2014). Impact of Hospital Variables on Case Mix Index as a Marker of Disease Severity.
Nurwahyuni, A. (n.d.). Performance of Private Hospitals under INA-CBGs Payment.
Sharma, M., Teerawattananon, Y., Luz, A., et al. (2020). Institutionalising Evidence-Informed Priority Setting for Universal Health Coverage: Lessons from Indonesia.
World Health Organization Indonesia. (2026). Indonesia Health Accounts 2024: Strengthening Evidence for Sustainable Health Financing.
Hidayat, B. (2024). Evolution of Health Technology Assessment in Indonesia.